The federal government says it is trying to prevent another opioid crisis.
It may be about to create one.
In July 2026, the Drug Enforcement Administration published a notice of intent to temporarily place 7-hydroxymitragynine above a specified threshold, commonly known as 7-OH, into Schedule I of the Controlled Substances Act.
Just days earlier, the DEA published a separate notice announcing its intent to temporarily schedule SR-17018, an experimental opioid compound that has gained attention among people trying to reduce their dependence on 7-OH and other opioids.
Think about what is happening.
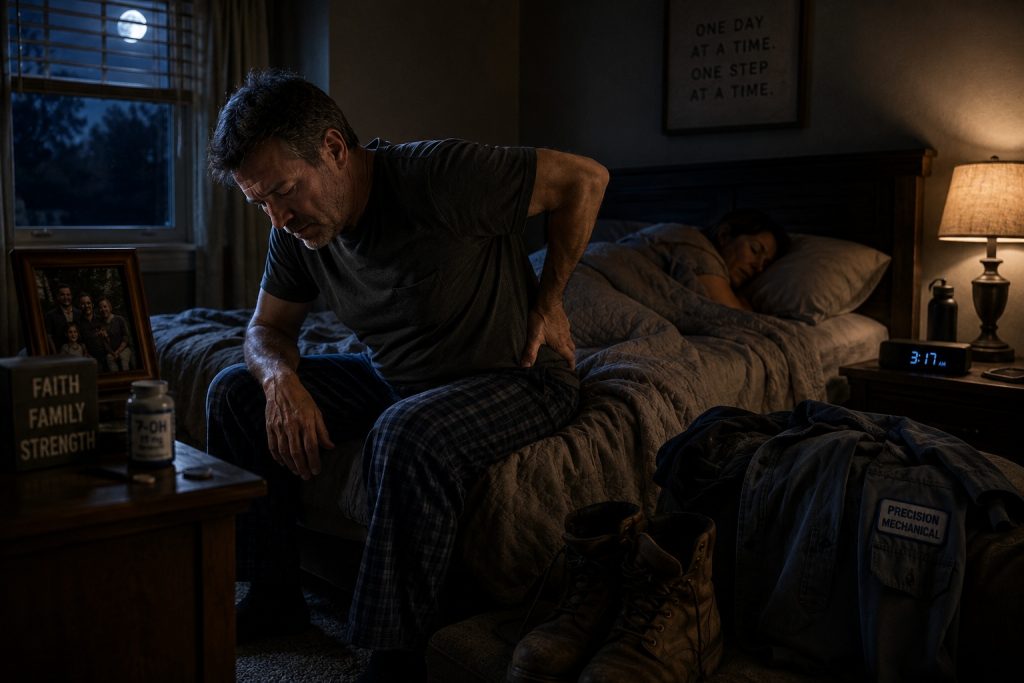
The government is preparing to ban a substance that thousands of people report using for chronic pain.
At almost the same time, it is preparing to ban an experimental compound that some dependent users report using to get off that substance.
This is not an argument that 7-OH is harmless.
It is not.
This is not an argument that today’s 7-OH market is responsible.
In many cases, it clearly is not.
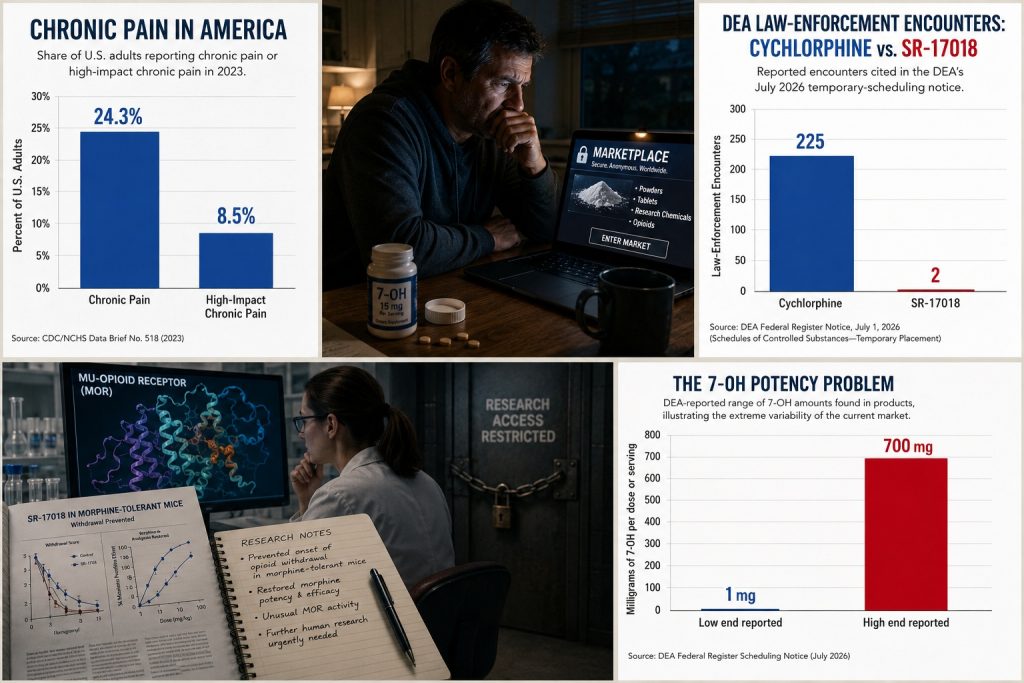
The DEA reports finding 7-OH products containing anywhere from 1 milligram to an astonishing 700 milligrams in a single dose or serving. Poison centers documented 165 7-OH exposure cases between January and July 2025. Among reported single-substance exposures, 35% resulted in serious health problems and 67% were treated at a healthcare facility.
Those numbers deserve attention.
But they also expose the actual problem.
The market is almost completely unregulated.
And instead of regulating it, standardizing it and forcing dangerous products off the market, the federal government has chosen the most extreme option available.
Schedule I.
The question is not whether 7-OH carries risks.
The question is whether banning it will save more lives than regulating it.
There is good reason to believe the answer may be no.
America Has a Chronic Pain Crisis Nobody Wants to Talk About
According to the Centers for Disease Control and Prevention, 24.3% of American adults experienced chronic pain in 2023.
Another 8.5% experienced high-impact chronic pain, meaning pain that frequently limited their life or work activities.
Nearly one in four American adults lives with chronic pain.
For millions of these people, pain is not an inconvenience.
It is their life.
It determines whether they sleep.
It determines whether they work.
It determines whether they can walk through a grocery store.
It determines whether they can play with their children or grandchildren.
It determines whether they can sit through dinner with their family.
It determines whether they want to wake up tomorrow.
At the same time, access to prescription opioid pain medication has declined dramatically.
The national opioid dispensing rate fell from 46.8 prescriptions per 100 people in 2019 to 35.4 prescriptions per 100 people in 2024.
There were legitimate reasons for reducing irresponsible opioid prescribing.
The pharmaceutical industry helped create a disaster.
Doctors were told that opioids carried a low risk of addiction.
Patients were placed on escalating doses.
Pill mills flourished.
People died.
We should never minimize what happened.
But the pendulum swung.
Today, many chronic pain patients say they cannot find physicians willing to manage severe long-term pain with opioids.
Doctors are concerned about addiction.
They are concerned about physical dependence.
They are concerned about regulatory scrutiny.
They are concerned about being accused of overprescribing.
And the patient is still in pain.
This is where policymakers repeatedly misunderstand people living with severe chronic pain.
Some of them are willing to accept physical dependence.
Physical dependence is not automatically the same thing as addiction or opioid use disorder.
A physically dependent patient may experience withdrawal if a medication is suddenly stopped.
That does not necessarily mean the person is compulsively using the drug despite harm.
For some chronic pain patients, the calculation is simple.
“If I have to take this medication every day for the rest of my life to function, I accept that.”
People who do not live with severe chronic pain may find that difficult to understand.
People who do live with it understand immediately.
When pain controls every waking hour of your life, the possibility of physical dependence may feel like a reasonable trade for the ability to work, sleep and function.
The CDC’s own 2022 opioid prescribing guideline emphasizes individualized care and states that patient values and preferences should be considered when making pain-treatment decisions.
Yet with 7-OH, the patient’s preference is about to become irrelevant.
The government is making the decision for them.
People Are Already Using Kratom-Related Products for Pain
We do not have reliable national data showing exactly how many Americans use concentrated 7-OH specifically for chronic pain.
That is an important limitation.
But we do have substantial evidence about why people use kratom-related products.
In a survey of 2,798 kratom users, 91% reported using kratom for pain.
The same survey found that 67% used it for anxiety and 65% for depression.
The DEA’s own 7-OH scheduling notice acknowledges that users report self-treating pain and anxiety with 7-OH. The agency also acknowledges online reports of people using these products for chronic pain.
That creates an uncomfortable contradiction.
Schedule I is reserved for drugs deemed to have no currently accepted medical use in the United States.
Legally, “currently accepted medical use” has a specific regulatory meaning.
Anecdotal reports do not establish an FDA-approved medical use.
Animal studies do not automatically establish accepted medical use.
That legal distinction matters.
But let’s stop pretending the legal definition answers the scientific question.
”No currently accepted medical use” does not mean “no medical potential.”
7-OH has demonstrated analgesic activity in preclinical research.
A study published in Life Sciences demonstrated antinociceptive effects of 7-hydroxymitragynine in mice and examined its opioid-receptor activity.
Later research showed that mitragynine can be metabolized into 7-hydroxymitragynine and that this active metabolite contributes to analgesic effects through the mu-opioid receptor.
None of this proves that the 7-OH tablets currently being sold online are safe.
It does prove something else.
The compound interacts with biological systems involved in pain.
People report taking it for pain.
Preclinical research demonstrates analgesic activity.
The government’s response should be clinical research.
Instead, it is Schedule I.
The Government Already Knows What Happens When Dependent Patients Suddenly Lose Access
This is perhaps the most frustrating part of the entire 7-OH debate.
We have already studied what can happen when physically dependent people suddenly lose access to opioids.
The federal government has warned doctors about it.
The Department of Health and Human Services specifically warns clinicians against rapid opioid tapering or sudden discontinuation in physically dependent patients.
Why?
Because abrupt discontinuation can cause acute withdrawal.
It can worsen pain.
It can cause serious psychological distress.
It can contribute to suicidal thoughts.
And HHS explicitly warns that patients may seek opioids from illicit sources to treat their pain or withdrawal.
Read that again.
The federal government already acknowledges that suddenly removing opioid access can push people toward illegal opioids.
The CDC also warns against abrupt discontinuation.
In fact, the 2022 CDC opioid guideline was partly designed to correct harmful misapplications of earlier prescribing guidance.
Research has found similar warning signals.
A Veterans Health Administration study found that patients faced an increased risk of death from overdose or suicide after stopping opioid treatment. The risk increased among patients who had received opioids for longer periods.
Another study found opioid tapering was associated with elevated risks of overdose, withdrawal and mental health crisis that persisted for as long as two years after tapering began.
These studies involved prescription opioids.
They do not prove that exactly the same outcomes will occur after a 7-OH ban.
But ignoring the comparison would be reckless.
The government is preparing to remove access to an opioid-like substance from an unknown number of physically dependent people.
Where is the transition plan?
What Will Happen When 7-OH Disappears?
Nobody knows exactly.
That is the problem.
The DEA cannot tell us how many Americans currently use concentrated 7-OH every day.
It cannot tell us how many are physically dependent.
It cannot tell us how many use it primarily for chronic pain.
It cannot tell us how many previously used prescription opioids.
It cannot tell us how many previously used fentanyl or heroin.
It cannot tell us how many will seek treatment.
And it cannot tell us how many will enter the illegal drug market.
Yet we are preparing to conduct a massive real-world experiment.
There are at least four predictable outcomes.
1. Many People Will Continue Using 7-OH
Passing a law does not eliminate demand.
A person with severe chronic pain does not wake up the morning after a scheduling order and suddenly stop hurting.
A physically dependent person does not stop being dependent because Congress or the DEA changed a drug’s legal classification.
Some people will continue buying 7-OH.
The difference is where they will buy it.
Today, many consumers purchase products from public websites and retail businesses.
These businesses have names.
They have addresses.
They accept credit cards.
They can be sued.
Their products can be purchased and tested.
Regulators can inspect them.
Bad actors can be identified.
Once the substance moves underground, those protections begin to disappear.
Some consumers will turn to encrypted messaging applications.
Some will use dark-web markets.
Some will buy from anonymous social-media accounts.
Some will buy powders imported from overseas laboratories.
People who originally sought pain relief may suddenly find themselves participating in an illegal drug market.
We will have criminalized them without curing their pain.
2. Some Will Turn to More Dangerous Opioids
This is the consequence policymakers should fear the most.
The American illicit opioid market is not the same market that existed 20 years ago.
It is saturated with fentanyl and increasingly unpredictable synthetic opioids.
In 2025, the DEA seized more than 47 million fentanyl-laced counterfeit pills and nearly 10,000 pounds of fentanyl powder.
The DEA estimated those seizures represented more than 369 million potentially lethal doses of fentanyl.
That is the illegal drug market waiting for displaced 7-OH users.
It would be irresponsible to say that “drug cartels are celebrating the 7-OH ban.” There is no evidence proving that.
But basic economics is not complicated.
If demand continues after a legal supply disappears, illegal suppliers have an opportunity.
The United States has seen versions of this before.
Restrict one source of opioids without adequately addressing demand and users may migrate toward substitutes.
The danger is especially severe for chronic pain patients who have no experience with illicit opioids.
A person accustomed to buying a labeled 7-OH tablet may have no idea how to evaluate an illicit powder.
They may not recognize a counterfeit pill.
They may not understand fentanyl contamination.
They may not know what a nitazene is.
They may not own naloxone.
They may use alone.
These are not experienced street-drug users.
Some are ordinary people who started taking a legal product because their back hurt.
The first counterfeit pill they take could also be the last.
3. Some People Will Die by Suicide
People will accuse anyone raising this concern of being dramatic.
The data say otherwise.
Chronic pain is associated with a substantially elevated risk of suicide.
A 2023 systematic review and meta-analysis found that approximately one in four people with chronic pain reported suicidal ideation within the previous two weeks, although the researchers noted substantial variation among the studies included.
Other research has estimated that the risk of suicide death among people with chronic pain is at least twice that of people without chronic pain.
Pain changes people.
Unrelenting pain changes how a person thinks about tomorrow.
Now imagine someone who has suffered for years.
They finally find something that allows them to function.
Maybe it is not perfect.
Maybe they have become physically dependent.
Maybe they wish they had never started taking it.
But they can get out of bed.
They can work.
They can sleep.
Then the government tells them it is disappearing.
Some will stockpile.
Some will taper.
Some will seek medical treatment.
Some will find substitutes.
And yes, some may decide that when their supply is gone, they are done.
We should not pretend this possibility is imaginary.
The FDA and HHS have previously warned about suicidal thoughts and suicide associated with abrupt or rapid opioid discontinuation in physically dependent patients.
A Veterans Health Administration study found increased overdose and suicide mortality after opioid treatment was stopped.
Again, these studies are not specific to 7-OH.
But the warning is impossible to ignore.
Before the government abruptly disrupts access for a physically dependent population, it should know how it plans to protect the most vulnerable members of that population.
Right now, where is that plan?
4. Emergency Departments Could See a Wave of Withdrawal Patients
Opioid withdrawal is often described as “not life-threatening.”
That statement is frequently repeated without context.
Unlike severe alcohol or benzodiazepine withdrawal, uncomplicated opioid withdrawal is generally not considered directly fatal.
But that does not mean it is medically insignificant.
Severe vomiting and diarrhea can cause dehydration and electrolyte disturbances.
Withdrawal produces intense autonomic stress.
Rare but potentially life-threatening cardiac complications, including withdrawal-associated Takotsubo cardiomyopathy, have been documented.
More importantly, withdrawal can drive relapse and return to opioid use after tolerance has changed.
That creates a significant overdose risk.
The DEA’s own Federal Register analysis notes increasing adverse-event reports involving 7-OH. Dependence and withdrawal are specifically among the reported problems.
If a large population loses access at approximately the same time, where will they go?
Many will go to emergency departments.
Others will call addiction treatment programs.
Others will seek urgent appointments with pain specialists.
We do not know the size of this population because the government does not appear to have reliable prevalence data.
That uncertainty should concern everyone.
Emergency department crowding is already a serious patient-safety issue.
Research has associated severe ED crowding with worse patient outcomes. One study found that occupancy above 90% was associated with increased 10-day mortality among non-critical patients.
It would be scientifically dishonest to claim that a 7-OH ban will definitely cause heart attack patients to die in waiting rooms.
We cannot prove that.
But healthcare systems operate with finite capacity.
A sudden influx of patients seeking withdrawal treatment does not create new emergency physicians, nurses or hospital beds.
Every public health intervention has downstream consequences.
Those consequences should be modeled before the intervention occurs.
“Put Them on Suboxone” Does Not Solve the Entire Problem
When concerns about 7-OH withdrawal are raised, one response appears repeatedly:
Put them on Suboxone.
For people with opioid use disorder, buprenorphine can be lifesaving.
It reduces illicit opioid use and mortality risk.
Calling it “just trading one addiction for another” is medically inaccurate and unfair to patients who have rebuilt their lives with medication treatment.
But there is another group in this discussion.
The chronic pain patient.
Remember why some people started taking 7-OH.
Pain.
If a patient enters treatment for 7-OH dependence and receives buprenorphine, managing withdrawal is only part of the problem.
What happens to the original pain?
Buprenorphine itself can have analgesic applications. The Department of Veterans Affairs has reviewed evidence supporting its use in some chronic pain patients.
But it is not a universal solution.
Not every patient’s pain responds to the same medication.
Not every physician is comfortable managing buprenorphine for chronic pain.
Not every patient who is physically dependent on 7-OH has opioid use disorder.
This distinction matters.
Withdrawal management and chronic pain management are not the same thing.
A patient can successfully stop 7-OH and still be left with the exact medical problem that led them to use it.
If that problem remains untreated, what happens next?
Now We Need to Talk About SR-17018
This is where the federal government’s strategy becomes even more difficult to understand.
On July 1, 2026, the DEA published a notice of intent to temporarily place four synthetic opioids into Schedule I.
One of them is 5,6-dichloro desmethylchlorphine, commonly known as SR-17018.
The DEA states that a temporary scheduling order may be published on or after July 31, 2026.
SR-17018 is an experimental mu-opioid receptor agonist.
It is not FDA approved.
There are no large human clinical trials proving that it safely treats opioid withdrawal.
Let’s make that completely clear.
SR-17018 is not a proven medication for 7-OH dependence.
But something extremely interesting is happening.
People in 7-OH communities are reporting using SR-17018 to get off 7-OH.
Some users describe dramatically reduced withdrawal symptoms.
Some claim they transitioned off heavy 7-OH use in approximately ten days.
Some call it a miracle.
Those are anecdotes.
Anecdotes are not clinical trials.
But anecdotes can identify research questions.
And in the case of SR-17018, there is already preclinical science that makes the reports difficult to simply dismiss.
A published study examining SR-17018 in morphine-tolerant mice found something remarkable.
When researchers substituted SR-17018 in morphine-tolerant mice, morphine potency and efficacy were restored while the onset of opioid withdrawal was prevented.
Read that carefully.
This was not an internet forum.
This was published preclinical research.
A later paper examining SR-17018’s unusual mu-opioid receptor activity specifically noted that the compound had been shown in preclinical animal models to prevent opioid withdrawal signs.
That does not prove it works in humans.
But it is a signal.
And when people independently begin reporting a similar phenomenon in the real world, the scientific response should be obvious.
Study it.
Immediately.
Instead, the DEA is moving to place it in Schedule I.
Look Closely at the DEA’s Own Numbers on SR-17018
The DEA’s Federal Register notice groups SR-17018 with three other synthetic opioids.
The agency reports 265 total law-enforcement encounters involving the four substances.
But those encounters were not evenly distributed.
According to the DEA’s own notice:
225 involved cychlorphine.
Only two involved SR-17018.
The notice also discusses 49 deaths involving cychlorphine.
Those 49 deaths were not attributed to SR-17018.
This distinction is extremely important.
When four compounds are grouped together in a scheduling notice, the reader may naturally assume that the strongest evidence of harm applies broadly to the entire group.
It does not.
The DEA does cite pharmacological concerns regarding SR-17018.
The agency states that available data demonstrate dose-dependent antinociception.
It also cites reports of users seeking SR-17018 for analgesic and euphoric effects and to reduce or reset opioid tolerance.
Those are legitimate reasons for concern and research.
But think about the evidence before us.
The DEA acknowledges antinociceptive activity.
Published animal research found SR-17018 prevented the onset of opioid withdrawal in morphine-tolerant mice.
Online users are reporting using it to reduce 7-OH withdrawal.
And the DEA reports only two law-enforcement encounters involving SR-17018 since 2025.
The government’s response is Schedule I.
Why?
Who Benefits From Banning SR-17018 Before We Study It?
This question will make some people uncomfortable.
It should.
Who benefits when a compound people can purchase outside the traditional medical system appears to help them reduce opioid dependence?
Who benefits if that compound disappears?
Who benefits when the only remaining options require prescriptions, clinical appointments and long-term pharmaceutical treatment?
These questions do not prove a conspiracy.
They should not be used to make unsupported accusations against pharmaceutical companies or government officials.
But asking who benefits from public policy is not conspiracy theory.
It is basic policy analysis.
Buprenorphine is an important medication.
Methadone is an important medication.
Pharmaceutical treatment has saved lives.
But if an experimental compound shows a scientifically plausible ability to affect opioid tolerance and withdrawal, we should investigate it regardless of who owns the patent or who stands to profit.
Imagine if SR-17018 does not work.
Clinical trials could demonstrate that.
Imagine if it is dangerously cardiotoxic.
Research could identify that.
Imagine if repeated use causes severe dependence of its own.
Research could show us.
But imagine the other possibility.
What if the preclinical withdrawal findings translate to humans?
What if researchers discover a modified version of SR-17018 that helps people transition away from opioids with significantly less withdrawal?
What if studying its unusual receptor activity leads to an entirely new class of opioid-dependence treatments?
We will never answer those questions by forcing the compound into anonymous underground laboratories and internet drug markets.
Schedule I Does Not Make Research Impossible—But It Raises the Barrier
Supporters of the scheduling action will correctly point out that Schedule I substances can still be researched.
That is true.
Research does not become legally impossible.
But Schedule I research involves DEA registration and controlled-substance requirements.
The DEA’s own notices state that Schedule I controls apply to research, instructional activities and chemical analysis involving scheduled substances.
Research institutions can navigate those requirements.
Major pharmaceutical companies can navigate those requirements.
Well-funded universities can navigate those requirements.
But every additional regulatory hurdle affects which compounds receive attention and how quickly research moves.
SR-17018 needs more research now.
Not ten years from now.
The United States remains in an opioid crisis.
We should be aggressively investigating anything that provides a scientifically plausible lead on tolerance, dependence or withdrawal.
We Regulate Alcohol. Why Is Regulation Impossible Here?
The CDC estimates that excessive alcohol use causes approximately 178,000 deaths every year in the United States.
Alcohol causes physical dependence.
Alcohol withdrawal can kill.
Alcohol contributes to liver disease.
It contributes to cancer.
It contributes to heart disease.
It contributes to violence.
It contributes to motor vehicle deaths.
Yet alcohol is legal.
Why?
Because the United States eventually learned that prohibition created its own set of disasters.
So we regulate alcohol.
You must be a certain age to purchase it.
Retailers require identification.
Businesses need licenses.
Alcohol content is labeled.
Products are manufactured under regulatory standards.
Sales can be restricted.
Companies can face penalties.
Drunk driving is criminalized.
We regulate behavior and the market.
Why is a serious regulatory framework for 7-OH treated as an impossible idea?
The DEA itself found products ranging from 1 milligram to 700 milligrams per serving.
That is insane.
No responsible 7-OH company should defend a 700-milligram serving.
No responsible advocate should pretend a market selling candy-flavored, high-dose opioid-like products at convenience stores is sustainable.
But the existence of reckless products does not prove that every dose of 7-OH must become Schedule I.
It proves the market needs rules.
Here Is a Better Solution
There is a middle ground between 700-milligram 7-OH products and federal prohibition.
It is called regulation.
1. Make 7-OH strictly 21 and older.
Every in-person sale should require government-issued identification.
Online sellers should be required to use independent age-verification services.
A checkbox asking “Are you 21?” is not age verification.
2. Require behind-the-counter sales.
7-OH should never be displayed next to candy, energy drinks or ordinary kratom powder.
Customers should have to request the product from an employee.
Retailers selling it should require a specific license.
3. Require aggressive warning labels and standardized instructions.
Every product should clearly state that 7-OH acts on opioid receptors and may cause physical dependence and withdrawal.
Labels should warn consumers against combining it with alcohol, benzodiazepines, opioids and other central nervous system depressants.
Products should contain standardized serving instructions.
Until better human data exist, regulators should examine conservative instructions limiting use to no more than once daily.
4. Require strict independent laboratory testing.
Every batch should be tested for identity and potency.
Testing should also examine heavy metals, microbial contamination, residual solvents and relevant alkaloid impurities.
Each package should contain a QR code linked to a batch-specific certificate of analysis.
Laboratories falsifying results should face severe penalties.
Manufacturers knowingly selling mislabeled products should face criminal consequences.
5. Establish a maximum serving size.
The era of 100-, 300- and 700-milligram servings needs to end.
Federal regulators should immediately examine an interim maximum serving range of approximately 10 to 20 milligrams of 7-OH per serving.
The permanent limit should ultimately be based on human pharmacokinetic, toxicology and clinical data.
But allowing hundreds of milligrams in a single serving while arguing the only alternative is Schedule I is a false choice.
6. Create purchase limits and track high-volume sales.
A person should not be able to walk into a store and purchase thousands of milligrams of concentrated 7-OH without restriction.
Reasonable transaction limits could reduce diversion and impulsive high-dose use.
7. Create a national 7-OH adverse-event surveillance system.
Hospitals, poison centers and manufacturers should use standardized reporting categories specifically for 7-OH.
Stop combining traditional kratom leaf, mitragynine extracts and concentrated 7-OH into vague “kratom-related” statistics.
They are not the same products.
Good policy requires good data.
8. Fund urgent human research into SR-17018.
Do not market it as a miracle drug.
Do not tell people it is proven safe.
Do not encourage uncontrolled self-experimentation.
Study it.
Examine its pharmacokinetics.
Examine respiratory depression.
Examine cardiac effects.
Examine dependence.
Examine withdrawal.
And specifically investigate the preclinical finding that SR-17018 prevented opioid withdrawal in morphine-tolerant animals.
The people reporting dramatic reductions in 7-OH withdrawal may be wrong.
Or they may be pointing researchers toward something extremely important.
Science should answer the question.
The Government Needs a Transition Plan Before the Ban Takes Effect
Before concentrated 7-OH becomes Schedule I, federal officials should answer a simple question:
What is the plan for the people already dependent on it?
Not a press release.
Not “seek medical treatment.”
A plan.
Emergency physicians need clinical guidance specific to 7-OH.
Poison centers need standardized protocols.
Addiction specialists need information about buprenorphine induction after high-dose 7-OH use.
Pain specialists need guidance for patients whose underlying chronic pain remains uncontrolled.
The government needs to estimate how many daily users exist.
It needs to identify geographic areas with the highest use.
It needs to ensure treatment capacity exists before access is disrupted.
Naloxone distribution should be expanded specifically among current 7-OH users because some may transition to illicit opioids.
And current users should be warned clearly:
If you stop using 7-OH and later return to opioids, changes in tolerance may increase overdose risk. Illicit pills may contain fentanyl or other potent synthetic opioids.
That warning could save lives.
This Is Not About Defending the 7-OH Industry
Some companies in the 7-OH industry helped create this situation.
Let’s say that clearly.
Selling extreme-dose products was irresponsible.
Marketing products with candy imagery was irresponsible.
Allowing products to reach minors was unacceptable.
Pretending 7-OH was simply “strong kratom” was misleading.
Failing to clearly warn consumers about physical dependence was wrong.
Companies that behaved this way gave regulators every reason to intervene.
But bad companies do not excuse bad public policy.
The government has a responsibility to consider what happens after a ban.
You cannot remove a substance from a physically dependent population and declare victory on the day the scheduling order takes effect.
The consequences begin the next morning.
When the pain returns.
When the withdrawal starts.
When the stockpile gets smaller.
When the first desperate person searches for a replacement.
When the first counterfeit pill arrives in the mail.
When the first chronic pain patient decides they cannot live this way anymore.
Those people matter too.
We Have Seen What Happens When Policy Ignores Demand
The United States has spent decades fighting opioids.
We restricted prescriptions.
We shut down pill mills.
We reformulated medications.
We arrested dealers.
We seized drugs.
And yet the illegal opioid supply became more potent.
Heroin gave way to fentanyl.
Fentanyl appeared in counterfeit pills.
New synthetic opioids continued to emerge.
In 2025 alone, the DEA seized the equivalent of more than 369 million potentially lethal doses of fentanyl.
Supply matters.
But demand matters too.
Pain matters.
Dependence matters.
Withdrawal matters.
Desperation matters.
If policymakers ignore those forces, the illegal market will not.
The 7-OH market needs intervention.
It needs strict regulation.
It needs dose limits.
It needs age restrictions.
It needs honest labels.
It needs legitimate laboratory testing.
It needs bad actors removed.
And people who are dependent need treatment options and a safe transition.
SR-17018 needs rigorous research.
What we do not need is another public health policy built around the fantasy that making a substance illegal makes the people using it disappear.
They do not disappear.
Their pain does not disappear.
Their physical dependence does not disappear.
Their desperation does not disappear.
Only the legal supply disappears.
And in America in 2026, we know exactly what kind of illegal opioid market is waiting to replace it.
This ban may be intended to save lives.


